Breastfeeding v formula: Should the state step in?

Whether a mother breastfeeds or formula-feeds is an intimately private decision. It's her body - her choice, and no one should apply pressure upon her choice, right? I disagree.
Choice is overrated
A major flaw of contemporary society is that we tend to put choice on a pedestal. You can never be made worse off by having options, because you can always turn them down right? In a culture where our conception of choice is so tied up with virtues of dignity and independence, the reluctance to deny someone the right to choose can be so strong that it overrides concern for the well-being of babies, the wider society and even the chooser herself.
For instance, it is impossible to predict with absolute certainty what specific harm formula feeding will inflict upon your specific baby. The risks associated with formula use (gut problems, allergies, diabetes, ear infections, etc) are difficult to quantify. Formula feeding is an uncertain gamble. Thaler and Sustein (2009) argue that uncertain risk diminishes the value of choice:
“When people have a hard time predicting how their choices will end up affecting their lives, they have less to gain by numerous options and perhaps even by choosing for themselves”.
Currently parents have the right to choose formula or breastmilk. However when the risks of a parental act are substantive yet indiscernible, it may pay to adjust parental rights to protect infant well-being. In fact the law is already starting to do this:
Parents have Responsibilities not Rights

Over the last few decades the law has made a subtle yet symbolic shift in the way it views parenting. Once parents had ‘parental rights’, now they have ‘parental responsibilities’. The child is no longer a chattel for parents to do with as they wish (at least in theory).
Modern law readily overrides the wishes of parents in a range of contexts, from medical care to health and safety. The courts will authorise action where it is in the best interest of the child and ultimately, the state can intervene and substitute its own decision in place of the parent. In this context, a law restricting formula to a prescription-only basis would not seem far-fetched. It would cater to the same welfare principle as other well-established laws.
We need a Cultural Makeover
Legal change drives societal change. Currently, there are undeniably a lot of mothers who have decided not to breastfeed or to quit breastfeeding for purely social or cultural reasons (see The Infant Feeding Survey 2010 for evidence of this). If we support their decision without question, then we are perpetuating the social and cultural attitudes that got them there in the first place.

Well, one of the best ways to resist temptations is to avoid them in the first place, but this works only up to a point. We can put that cake back in the fridge rather than leaving it in plain sight on the counter to tantalize us, for example, but we can’t completely escape. If we’re bound and determined to go for seconds (or more), the only way to resist giving in is to be bound by a power beyond ourselves. The same goes for formula. We can resist the temptation to purchase a tub during pregnancy ‘just in case’, but when our baby arrives, and is screaming at 3am, it would only take a short trip to the store to sabotage breastfeeding. In the free market, formula is always available, like a proverbial carrot on a string. And most of the time, mothers are too exhausted, too stressed, and too ignorant to resist its allure. In this sense, contemporary society’s choice-worship reflects a certain naivety about the effects that context has upon choice. So what can we do about the insidious and undermining temptation of formula?
Solution #1: Formula on prescription

For the minority of women who genuinely can’t breastfeed (those with insufficient glandular tissue, those on incompatible life-saving medication, those that have had mastectomies for example), we could provide a safety net: formula on prescription. This would actually be far more sympathetic and equitable than the present state of affairs. Currently women who cannot breastfeed, through no fault of their own, still have to purchase formula at inflated prices. They are essentially being made to pay for their misfortune. “Formula has amongst the highest mark-ups on the supermarket shelves” (Baby Milk Action 2010). Placing formula on prescription will protect these mothers more than our system currently affords. Formula is after all, a ‘medicine’. It was created as an answer to limited cases of pathology. It's only logical that this life-saving medicine be placed on prescription, like the insulin that diabetics need for survival.

But wait, there’s more: We could enhance this process by installing a mandatory ‘cooling off period’. I take my inspiration from marriage law. Many countries impose a mandatory waiting period before a couple may get divorced. Asking people to pause and think before making a decision of that magnitude seems like a sensible idea, no? Aware that people might act in a way that they will regret, legislation does not block their choices altogether but does ensure a period of sober reflection. The same can be applied to the scenario of breastfeeding cessation:

Thaler & Sunstein 2009 support my analysis. They note that mandatory cooling-off periods make best sense, and tend to be imposed, when two conditions are met:
(a) People make the relevant decisions infrequently and therefore lack a great deal of experience; and
(b) Emotions are likely to be running high.
These are circumstances in which people are essentially prone to making choices that they will regret. I believe these two factors perfectly describe the breastfeeding scenario, and my assertion is supported by evidence: “90% of mothers who stop breastfeeding in the first few days and weeks would have liked to continue” (The Guardian 2011). There is obviously a lot regret and guilt flying around. So restrict formula to prescription and Vola! Essentially we can spare mothers of guilt by policing, or even removing, their choices! Case closed.

Oh drat!
So back to the drawing board...
If eradicating mothers’ easy access to formula by limiting it to prescription smacks of totalitarianism and goes against your democratic spirit of choice, what is an alternative solution? After all, babies are getting sick as a consequence of formula-use which is placing an undue burden on our health care system, not to mention the damage formula-use wreaks on the environment, alongside inflicting a host of other undesirable damages on society (I outlined all the social costs of formula-use here). How can we drive up breastfeeding rates in a politically more palatable way?
Solution #2: Taxation.
Although the prescription-only route would be a practical and equitable solution for those who genuinely can’t breastfeed, it would be impractical and inequitable for everyone else. Alas, it would be excessively radical. So how about we turn to a less-radical concept, one that everyone is familiar with – taxation!
Tax the formula companies?

We all know formula companies are shy on corporate responsibility, to put it mildly! Thus I initially thought the most appealing form of taxation would be aimed at these surreptitious corporations. Legislation could be passed demanding that formula companies transfer a proportion of their profits over to the state, a kind of corporate tax. The state could then spend this money on redressing the harms brought about by formula use – the environmental decay, the burden on the health care system, and so on.
However, as appealingly retributive as this sounds, it would be unlikely to have any effect on breastfeeding rates. Babies would still be consuming formula, consequently their health would remain sub-par. A corporation tax would not increase the numbers of babies being breastfed. Hmmm...so what is the solution?
The solution is simple, and what’s even better – the solution has already been road-tested many times before and proven to be successful in a range of health-related contexts! To increase breastfeeding rates we need to take a ‘bottom-up’ approach. In other words, target the parent!
But let’s not target the parent with health promotion messages or guilt trips - those tired strategies have been failing for decades. It seems that when babies’ health is concerned, factual and emotional incentives are insufficient. Knowing that formula feeding puts their child at increased risk of asthma, allergies, gastrointestinal infections, obesity, lower IQ, SIDS, et al – does not seem to be enough to incentivise parents to breastfeed. The incentive to formula feed is stronger.
When incentives are badly aligned, it is appropriate for the state to try to fix the problem by realigning them. Soooooo...
Tax the parents!

Instead of targeting parents’ moral consciousness (their hearts), we need to target parents’ financial sensibilities (their wallets). We do this by placing a tax on formula – a “sin tax” if you will. People value cold hard money over theoretical health. The immediate utility that results from money is not the same as that which arises from health which is more remote and prospective. Thus, a tax would be more incentivising than health messages alone.
And when our goal is incentivisation, it makes sense to target parents rather than formula companies. Parents are the decision-makers. They are the gatekeepers of their baby’s destiny – whether their offspring receives formula or breast milk is the consequence of parental action. I appreciate that taxing parents is controversial. Formula companies are after all, the big guys. They are billion dollar corporations with deeper pockets from which tax could be extracted. However - and this is the important part – formula companies do not make the final decisive act. It is not the formula company which fills the bottle and administers it to the baby. If we are to embrace the pro-choice rhetoric, we must appreciate that it places the consumer as a responsible agent, at the core of the consumption-decision.
 |
| It is not the formula company which fills the bottle and administers it to the baby. |
A tax on formula would also benefit society. At present, those who purchase formula do not pay the full costs that they impose on society, and the babies (the passive end-users) who stand to be harmed by formula lack any feasible way to negotiate with the purchaser to get them to clean up their acts.
A sin tax means that those who choose to formula feed will be paying for the consequences of their choice: the tax will cover the costs of their babies’ increased health care needs and the costs of repairing of the environmental damage. In essence, taxing the purchasers of formula will reduce its societal costs.

Let’s take an additional example from another health-related domain: a recent study found that smokers were actually happy when the cigarette tax was raised! Are smokers mathematically challenged? Do they have money to burn? No, they realize that a higher tax means more expensive cigarettes, and they don’t want to pay extra. So what’s going on? Well, smokers and potential smokers know they shouldn’t smoke. In both medical and financial terms, it’s a poor choice, dare I say just like formula-use! The incentives to not smoke, however, aren’t compelling enough to them. But when cigarette prices rise, the incentives to quit rise, and that’s a good thing. Likewise, when formula prices rise, the incentives to breastfeed rise. At some point, mothers decide they simply can’t afford to formula feed and go down the relactation or donor milk route. If they are pregnant, they might never formula feed.
There’s a snag though... taxes may be less restrictive than formula on prescription but they can still induce reactance if raised too high. I can see it now. A thriving black market of infant formula, men in oversized anoraks hanging on street corners with Aptamil tucked into their armpits. The threat of the black market is why it is vital that the tax be kept high enough to incentivise breastfeeding but low enough to protect from reactance. There’s an art to taxation. Too little is ineffective, while too much is counterproductive.

Sadly, the ultimate achilles heel of taxing formula users is that whilst it may incentivise some women to breastfeed, for those who still don’t want to, they remain at the mercy of the formula companies. These multi-national corporations control the nutritional content, price and availability of formula. They manipulate and monopolise not just parents, but health professionals and the market itself. We could tax the crap out of parents but it would not address the inherent lack of corporate responsibility in formula production. So now what?
Back to the drawing board!
Solution #3: Recompense breastfeeders

What’s better than taxation? The opposite of taxation – reward! By breastfeeding, a mother is not only preserving the optimum health of her baby and herself, she is also saving money for the state and protecting the environment to boot! She is benefiting us all. It is only reasonable that she should be rewarded for this diligence. Indeed, defensive formula feeders and associated whingy-pants argue that breastfeeding is not ‘free’ contrary to some lactivist assertion. They gasp: "Breastfeeding is only free if a mother's time is worth absolutely nothing" (Noonan 2012). So I propose that breastfeeding mothers be recompensed for their commitment.
Here’s how it would work in practice:
When a baby is born the state puts money into a ‘trust fund’. Once the mother can prove she has breastfed for 6 months/1 year/designated goal, she gets the money. If she fails, the money goes to a breastfeeding charity. The mother also has the option of entering into a group financial commitment with other mothers, in which the group’s pooled money is divided among those members of the group who reach their breastfeeding goals. This enhances the group members' drive to support each other. Strengthening female solidarity would be a welcome tonic in the current ‘mommy wars’ climate, no?

The same strategy can be applied to breastfeeding: a mother can receive a dollar a day for every day she breastfeeds her baby. This approach would feed into the mantra favoured by many contemporary breastfeeding advocates that ‘every feed counts’. By drawing the mother’s attention to breastfeeding as a day by day process the mother’s enthusiasm and commitment can be more easily retained.
So, why has the state never installed a recompense scheme for breastfeeding mothers? Is the lack of financial recognition of breastfeeding a sign of our patriarchal society yet again, overlooking and undervaluing women's work?
Well, yes and no. Sadly, whilst such a scheme looks good on paper, a recompense scheme would be unworkable for breastfeeding. How would mothers prove they were still breastfeeding successfully? Those who had failed would be incentivised to lie. Short of demanding stool samples from every alleged breastfed baby (a time-hungry, costly, not to mention stinky task) it would be difficult to distinguish a genuine breastfeeder from a fraud.
Therefore if disincentivization through taxation is undoable, and incentivisation through reward is undoable, perhaps focusing on motivation is not the remedy for dwindling breastfeeding rates. So what is?
Solution #4: Nationalise formula production
A final solution, and in my opinion, the most practical and equitable would be nationialising formula production.
na•tion•al•ize [nash-uh-nl-ahyz]
*verb*
to bring under the ownership or control of a nation
Bringing formula production under the control of the state would have notable advantages. So notable in fact, to be revolutionarily! Indeed, I am confident that nationialising formula production will reduce the overall demand for formula. And here’s how:

The goal of formula companies’ marketing strategy is to expose mothers to their products through as many different media as possible, influencing them on multiple levels, thus taking advantage of what psychologists call the ‘mere exposure effect’. Essentially, the more we are exposed to a particular object or idea, the more we like it! Scientific recognition of this phenomenon took hold in the 1960s, when a series of laboratory experiments demonstrated that simply exposing subjects to a familiar stimulus led them to rate it more positively than other, similar stimuli which had not been presented. In fact, so innate is this behavioural response that it applies to both the human and animal kingdoms! Essentially, the mere omnipresence of formula increases its desirability. When you compare the strong presence of formula in our culture to the weak presence of breastfeeding, it is hardly surprising that our breastfeeding rates are so pathetic. Formula saturation is not only a symptom of the problem – it is the problem.


Formula companies spending so much on advertising and promotion is one of the reasons that formula is currently so expensive. The companies plough all this money into marketing for one reason only: it works! Mike Brady Campaigns and Networking Coordinator at Baby Milk Action has remarked: “It makes me very sad when I see parents repeating the misleading claims about a brand - doing the company’s advertising job for it - particularly when this leads to parents paying out more money than they need to.”

Under nationalisation there would be one generic state-owned ‘brand’ with no marketing influence. Formula packaging would be plain and contain only relevant information. Here is an example of a generic formula label that could be used under my proposed nationalisation scheme. It was created by Emergency Nutrition Network an international group of humanitarian agencies:
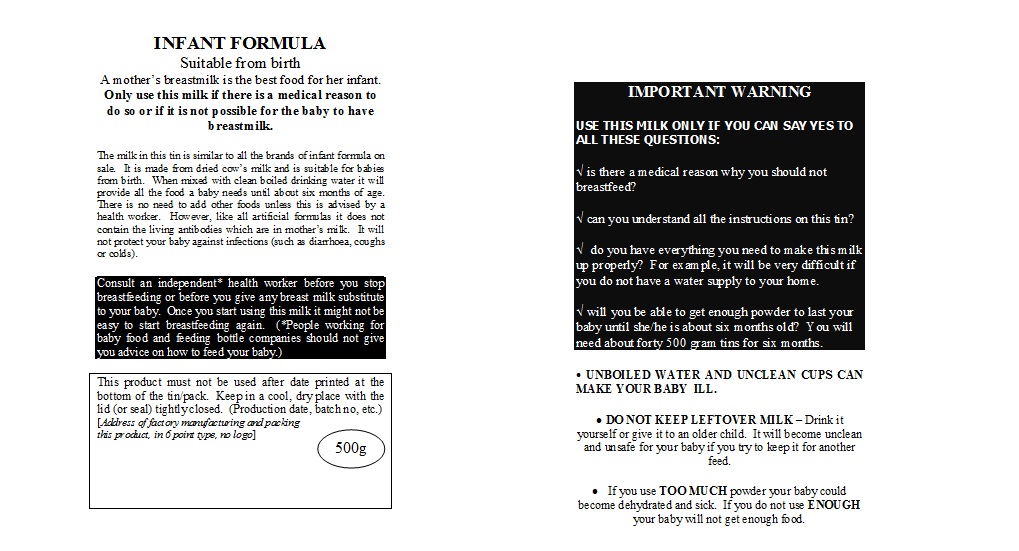

Break the marketing > demand > marketing chain by nationalising formula, and you will see a radical drop in demand along with better informed mothers. Mike Brady agrees:
“My view is we should treat formula for what it is: a nutritional medicine. Get rid of the polar bears and bright colours, free gifts and baby clubs, and have it available for those who need it, but without the hype.”

What are your thoughts? Is nationalisation the answer? Do comment below, or debate on the Facebook group.



Comments
Post a Comment