Timeline of Childhood Illness
Jump to age...
Newborn:
 |
| Stages of umbilical cord healing. |
- Umbilical Cord Problems: After a baby is born, the umbilical cord, which connected the baby to the placenta, is cut. In the majority of cases, the cord stump heals without problems but it can become infected or a collection of scar tissue (called a granuloma) may form. Until the cord stump has finally healed, infection can occur as the moist area around it can harbour potentially harmful bacteria. The exact cause of granuloma is not known but it may be more likely to occur if healing takes longer than usual. They usually disappear on their own, however if you suspect infection, see your doctor who may prescribe an antibiotic cream.
- Bloodshot Eyes: This is a harmless condition that occurs when there is trauma to the eyeball - often in the form of broken blood vessels - during vaginal delivery. Like a skin bruise, the discolouration disappears in a few days and does not indicate there has been any damage to your baby's eyes (Murkoff 2010).
- Erythema Neonatorum: It is common for newborns to develop this blotchy rash over the face and body. It is not known why it occurs, but it tends to get better within a few days without treatment (Kenny 2013).
- Milk Allergy: Milk allergy is when your baby's immune system reacts to proteins in milk. It is the most common childhood allergy, affecting between two per cent and seven per cent of babies. Babies who have eczema are more likely to suffer from it (Sicherer 2013). Your baby can take in milk protein through your breastmilk if you have drunk or eaten dairy produce, or she might react to cow's milk-based formula milk. Babies can be allergic to casein in milk (the curd formed when milk turns sour), the whey (the watery part left when the curd is removed), or both. Symptoms include nausea, abdominal pain, bloating and diarrhoea. Breastfeeding mothers can alter their diet to address the symptoms (read two mothers’ stories here and here). Most children will have grown out of their milk allergy by the time they are three. Milk allergy is not to be confused with lactose intolerance which is when your baby has difficulty digesting the lactose, or the sugar, found in milk. This is much rarer than milk allergy.
- Bacterial Conjunctivitis: This is inflammation of the conjunctiva, the transparent membrane that covers the white part of the eye and the inner eyelids. Newborns sometimes develop bacterial conjunctivitis as a result of infection from the mother as they pass through the birth canal. Most cases of bacterial conjunctivitis are mild and do not require medical treatment as they get better within a few days. Several studies have shown that dispensing colostrum into the baby’s affected eye can speed up the recovery process (Singh et al 1982; Ibhanesebhor and Otobo 1996; Verd 2007; Baynham 2013).
- Cephalhaematoma: This is the medical term which describes a fluid-filled swelling on the head when occurs in some babies. During delivery, one of the blood vessels that lies on the outside of the skull bones ruptures due to the twisting forces. When it bleeds the blood is trapped between the bone and its strong outside covering, which leaves a prominent fluid-filled lump. This lasts anywhere from one month to six months and is nothing to worry about (Green 2010).
- Neonatal Jaundice: In jaundice, the skin and eyes have a yellowish tinge. It is common in newborns, effecting about 6 out of every 10 babies, and is not usually serious (NICE 2010). The yellow tinge is due to a build-up of bilirubin in the blood. Bilirubin is a waste product formed by the liver when red blood cells are broken down. Newborns have more red blood cells and the removal of bilirubin from the blood is slower than in adults as their livers are immature.
- Hydrocele: Newborn baby boys are sometimes born with a hydrocele. This is a collection of fluid within the scrotum, the sac that encloses the testes. Many hydroceles improve with time, and often no treatment is required. If your son’s hydrocele has not disappeared by the age of 1 or is very large and causing discomfort, it can be surgically removed (Kenny 2013).
- Hip Dislocation: One baby in about 250 is born with congenital hip dislocation (Valman 2013). In this condition, the head of the femur (thighbone) lies outside the socket of the pelvis or is unstable and is likely to slip out of position. Babies are screened for congenital hip dislocation soon after birth, and tests for the condition are included in routine check-ups during the first year of life. Congenital hip dislocation runs in families and is more common in girls than in boys (NHS 2006).
- Hypospadias: In this congenital abnormality, which affects boys, the opening of the urethra is located on the underside of the penis rather than at the tip. Hypospadias is detected during the routine physical examination that is done on all newborn babies. It is usually corrected by an operation that is performed before a boy is 2 years of age (Bupa 2012).
- Clubfoot: This is a congenital deformity, also known as talipes, in which the foot is twisted out of shape or position. Clubfoot affects three times more male than female babies, and in half of all cases, both feet are affected (NHS 2013). Postural clubfoot is caused in the womb when the position of the baby’s foot forces it to be compressed. Unusually large babies are prone to this. Structural clubfoot is caused by an inherited abnormality of the bones in the foot. Structural clubfoot will require treatment.
- Hydrocele: This painless swelling of the scrotum occurs when fluid accumulates in the space around the testis. Hydroceles are very common in newborn babies, and they usually disappear without treatment by the age of 6 months (Chang et al 2010).
- Tongue-Tie: One in 10 babies are born with tongue-tie, a condition which can prevent them from breastfeeding effectively (Dillner 2011). Tongue-tie, also known as ankyloglossia, is a congenital oral anomaly which can decrease mobility of the tongue tip. It is caused by an unusually short, thick lingual frenulum, a membrane connecting the underside of the tongue to the floor of the mouth. Tongue-tie varies in degree of severity from mild cases characterized by mucous membrane bands to complete ankyloglossia whereby the tongue is tethered to the floor of the mouth. If feeding is affected, the tongue-tie needs to be divided. This involves cutting the short, tight piece of skin that connects the underside of the tongue to the floor of the mouth. It is a simple and painless procedure that usually resolves feeding problems straight away.
- Blue Baby: Babies may have mildly blue hands and feet, but this may not be a cause for concern. If their hands and feet turn a bit blue from cold, they should return to pink as soon as they are warm. Occasionally, the face, tongue, and lips may turn a little blue when the newborn is crying hard, but once he becomes calm, his color in these parts of the body should quickly return to normal. However, persistently blue skin coloring, especially with breathing difficulties and feeding difficulties, is a sign that the heart or lungs are not operating properly, and the baby is not getting enough oxygen in the blood. Immediate medical attention is essential



1 Week:
- Milia: Milia is a rash of tiny creamy white spots that may appear on the nose and cheeks of a newborn around now. The spots occur because the baby’s sebaceous glands are not well-enough developed to function properly. They remain until the sebaceous glands mature, usually within the first three months (Zuniga et al 2013). The spots are not itchy and give rise to no unpleasant symptoms in the baby.
- Diaper Rash: Diaper or nappy rash affects most babies and toddlers at some point but is particularly troublesome in the early weeks because baby’s skin is so sensitive. It is most commonly caused by irritation of the skin from the ammonia in urine and faeces. Using cloth diapers can help reduce the risk of diaper rash because many babies are sensitive to the plastics in disposable diapers (Erasala 2011). Diaper rash can also be caused by a fungal infection. If a barrier cream does not help, see your doctor who may prescribe a low-dose steroid anti-inflammatory cream, or for an infection, some antibiotics.
- Balanitis: This is the inflammation of the tip of the penis. It can be caused by diaper rash or by an allergic reaction to the soap powder in which your baby’s clothes are washed. The condition is not serious but a doctor should be consulted so that an antibiotic cream can be prescribed if necessary.
- Abdominal Distension: Most babies’ bellies normally stick out, especially after a large feeding. Between feedings, however, they should feel quite soft. If your child’s abdomen feels swollen and hard, and if he has not had a bowel movement for more than one or two days or is vomiting, call your doctor. Most likely the problem is due to gas or constipation, but it also could signal a more serious intestinal problem (Sullivan 2012).

2 Weeks:
- Neonatal Acne: This usually appears around 2-4 weeks after birth and is due to the effects of hormones from the mother when the baby is developing in the womb. These hormones stimulate the oil-producing glands in the baby’s face. The spots clear up on their own by 4-6 months (Baldwin 2014).
- Constipation: Bowel habits vary among babies: some pass a stool several times a day, others twice a week (see ‘Timeline of a Breastfed Baby’). Both are normal. A baby is constipated if she starts to pass stools that are hard, dry and difficult to pass. Formula fed babies are more likely to develop constipation (Quinlan et al 1995). Constipation often only lasts a few days. If it lasts longer, see your doctor.
- Oral Thrush: Babies can develop a yeast fungal infection in their mouths, known as oral thrush. The same fungus (Candida albicans) can also affect the diaper area, and lead to the development of diaper rash. Oral thrush is most common in babies up to 10 weeks but can affect older babies too. If you suspect your baby has oral thrush, take her to the doctor who can prescribe antifungal gels or drops. It is important to seek speedy treatment, particularly if you are breastfeeding, as oral thrush can cause breastfeeding issues (see here).
- Umbilical Hernia: During development in the womb, there is a period when some of the intestines lie within the umbilical cord, outside the abdomen. Normally they return to the abdomen and the abdominal wall has closed by the time of birth. In an umbilical hernia, part of the intestines protrudes through a weakness where the wall has not closed completely causing a bulge at the navel. An umbilical hernia usually appears 2 to 3 weeks after birth. Umbilical hernias are common in babies: about 1 in 10 are affected (NHS 2013). In the majority of cases no treatment is needed as the muscles seal themselves and the hernia disappears by the time the child is one year old.
 |
| Neonatal acne. |
 |
| Oral thrush. |

1 Month:
- Cradle Cap: Also known as seborrhoeic dermatitis, cradle cap is a common skin condition that usually develops in the first few months after birth. The cause of cradle cap is unknown, but it may be due to the effects of the mother’s hormones in the womb stimulating the sebaceous glands to become overactive and produce too much of the oily substance sebum. On the scalp, this causes dead skin cells to stick to the scalp instead of flaking off as normal. Cradle cap is not caused by poor hygiene and is not contagious. It does not cause any problems or pain to the baby and tends to clear up on its own, generally in a few months (Kern 2012).
- Disarticulated Skull: During birth a baby’s head is compressed and moulded to fit through the birth canal. After delivery the head starts to ‘un-mould’, but in some cases this doesn’t always happen quickly, especially if the delivery was assisted (Mackonochie 2007). This can lead to the nerves in the skull being irritated, so that the baby becomes fractious as a result. Cranial osteopathy, a gentle touch therapy, can be used to decompress the joints in the skull so that the baby gets relief and becomes more comfortable and settled.
- Wind: Wind is air in your baby’s digestive system, some of which is swallowed during feeding or crying. Wind can cause discomfort or pain and can make babies feel full so they do not feed properly. It can also cause vomiting. Baby massage can help relieve the symptoms. Infacol, Colief or Gripe Water are unnecessary (see ‘Timeline of Parenting Products You Don't Need’).
- Inguinal Hernia: In an inguinal hernia, weakness in the abdominal wall causes part of the intestines to bulge out, producing a lump in the groin. Most inguinal hernias occur in boys, with up to 1 in 50 being affected, and they are more common in premature babies (NHS 2013). In most cases, an inguinal hernia will be diagnosed at the baby’s 6 week checkup. Elective surgery to repair the hernia is recommended to prevent the risk of it becoming irreducible.
- Squint: When a child has a squint, one eye looks forward and the other eye looks in a different direction. A squint is caused by an imbalance of the eye muscles that control the direction of eye movements. Squints are extremely common in babies but should settle by the time the baby is 3 months old. Sometimes it can look like a baby is squinting because of the shape or their face and eyes, but in fact there is not a squint. This is called pseudosquint and is not a cause for concern. If a baby’s squint persists into toddlerhood, it is important to seek treatment promptly to prevent the development of vision problems.


2 Months:
- Sticky Eye: Your baby's tears don't start flowing until the end of their first month. That's when the fluid that bathes the eye is produced in sufficient quantity by the glands over the eyeballs. The ducts are particularly minute in babies and this makes them prone to blocking. A symptom of blocking is pus or discharge coming from one or both eyes, causing the eye or eyes to become sticky. The discharge may be more obvious after the baby has been asleep when there may be some crusting around the eyes. Normally, blocked ducts are nothing to worry about and clear up by themselves by the end of the first year, however it is wise to see your doctor to rule out conjunctivitis (Murkoff 2010).
- Penile Adhesion: This is a possible reaction to circumcision. Whenever tissues of the body are cut, the edges will stick to the surrounding tissue as it heals. After the foreskin of the penis is removed during a circumcision, the circular edge remaining tends to stick to the penis as it heals. If a significant amount of foreskin remains after the circumcision, it, too, can stick to the penis during the ealing process, causing the foreskin to reattach (Murkoff 2010).
- Reflux: Reflux occurs when the stomach contents come back up into the oesophagus or even into the mouth. The condition, also known as gastro-oesophageal reflux, usually starts in the first few months of life. It is caused by immaturity of the muscle, or sphincter, between the oesophagus and stomach. Most babies grow out of it, however if the symptoms are severe, see your doctor. You can read mothers' experiences of having reflux babies by clicking here and here.
- Colic: While all babies cry at some point for various reasons (see ‘Timeline of Challenging Early Childhood Behaviour’), babies with colic cry inconsolably for unknown reasons. It is thought that colic may be caused by trapped wind or with immaturity of the digestive system because it tends gto disappear when baby is around 3 months old. It may also be caused by a temporary sensitivity to lactose. Colic is extremely common, and effects about 1 in 5 babies (Kaye 2012). Baby massage and a warm bath can help to relieve the symptoms of colic. Failing this simeticone drops or lactase drops may help.
- Undescended Testes: When in the womb, boys’ testes develop within their abdomens, moving down into the scrotum towards the end of pregnancy. One or both testes sometimes fail to descend before birth. During your baby’s 6-8 week checks, your doctor will check the scrotum to see if the testes are in the correct place. If your doctor cannot feel a testis, they will ask you to bring your baby back for another examination when he is around 3 months old, as many boys’ testes descend into the scrotum at around this time (Wright 2012).
 |
| Sticky eye, not to be confused with conjunctivitis. |
 |
| Illustration showing what happens during reflux. |
 |
| Undescended tesicle shown on the left. |
3 Months:
- Hair Loss: Between 3 and 6 months of age, many babies have a bald spot resulting from friction with the crib mattress or car seat. This is because young baby hair is not very firmly embedded in the scalp and only a small amount of friction is needed to rub it loose. Once your child starts sitting up, any lost hair should return.
- Roseola Infantum: This viral illness affects children aged 3 months to 3 years. It is caused by breathing in droplets from an infected child, and symptoms begin 5-15 days after infection. Symptoms include a fever lasting for about 3 days, swollen lymph glands in the neck, a sore throat and earache. Roseola infantum is usually very mild and most children recover from it very quickly. Most children will have caught roseola infantum by the time they are 2 years old (Collins 2009).
- Oral Thrush: The main symptom of oral thrush is one or more white spots or patches in your baby's mouth. The patches can look like curd or cottage cheese. Oral thrush is common in babies and there are several antifungal gels that can treat it. It is important to see your doctor if you suspect your baby has oral thrush as it can cause pain during breastfeeding.
 |
| Normal infant baldness. |
4 Months:
- Slapped Cheek Syndrome: This viral infection, also known as fifth disease or erythema infectiosum, causes a distinctive red rash on both cheeks. The infection that causes slapped cheek syndrome, parvovirus B19, is spread by breathing in droplets from infected people’s coughs and sneezes (NHS 2011). Symptoms include a fever, sore throat, tiredness and feeling unwell followed 3-7 days later by the rash. It is generally a mild, short-lived illness.
- Thalassaemia: This is a form of genetically inherited anaemia. It occurs mostly in people from the mediterranean area but it can also affect people from India and south-east Asia. Thalassaemia can be passed on to a child if both parents carry the faulty gene. The parents themselves may not be anaemic but there is a one in four chance that their child will suffer from the disease. If he does, his body cannot make normal haemoglobin, the substance in the blood that makes the red cells red and carries oxygen through the body. The problem reveals itself when the child is around 4 months old with symptoms of severe anaemia: fatigue, breathlessness and pallor; he will then become increasingly inactive. A child with thalassaemia will also have difficulty feeding, and his abdomen will become swollen as the spleen and liver enlarge. A less severe form of the condition, called thalassaemia minor does not cause these symptoms and requires no treatment.
- Flattened Head Syndrome: Also known as deformational plagiocephaly or plagio, flattened head syndrome occurs when pressure causes the soft bones of the head to become flattened. In most cases it rights itself as the child gets older.
 |
| Slapped Cheek Syndrome. |
5 Months:
- Heat Rash: Heat rash commonly affects babies of this age because they still have difficulty regulating their temperature and yet tend to start wearing layered outfits. Simply removing some clothing can help. Moving the baby into the shade or a cool area can also help.
- Inhalation of a Foreign Body: A rapid onset of whistling or a wheezing sound heard on breathing in a child not known to be ill could be a sign that he or she has inhaled a foreign body, causing it to lodge in the windpipe or trachea. The child may appear calm. On the other hand, enhaling a larger foreign body, such as a small coin or marbel, will probably cause the child to wheeze, cough and be distressed. They may also have a bluish tinge to the nose, ears and lips. This is called cyanosis and is always a medical emergency (Dugdale 2013).

6 Months:
- Teething: Teething usually starts at around 6-9 months. The bottom two middle teeth generally come through first, then the top front teeth, followed by the others, with the back molars last (see diagram). Some babies go through teething without seeming to suffer any discomfort and the first you notice about teething is when the teeth appear. Others find it a painful experience and may have symptoms for months before a tooth emerges. Baby led weaning can help ease the discomfort cause by teething as it allows baby to chew on the food at their own pace (Edwards 2002). Cucumber, apple or frozen banana makes a soothing, healthy snack.
- Coeliac Disease: Babies with celiac disease are sensitive to gluten, a protein found in wheat, rye, and barley. Eating these foods leads to symptoms such as abdominal pain and bowel upsets. They may also react to a similar protein found in oats. The condition is not an allergy to gluten, but an autoimmune disease in which the body mistakenly attacks itself (NICE 2009).
- Malabsorption: Malabsorption is the result of the small intestine’s failure to absorb adequate nutrients, such as vitamins, minerals, fats and amino acids, from food. The problem is always associated with an underlying condition. Malabsorption is sometimes caused by damage to the lining of the small intenstine, which interfers with the intestine’s ability to absorb nutrients from food. Malabsorption may also be due to a deficiency of the enzymes involved in digestion, which prevents the breakdown of foods into units small enough to be absorbed. Symptoms of malabsorption include diarrhoea, loss of weight and failure to put on weight, and listlessness. If your baby shows any of these signs, alert a medical professional.
- Eczema: In this skin condition the skin becomes dry and itchy. Atopic eczema is the most common type in infants, with as many as 1 in 5 developing it (Collins 2009). Atopic refers to a sensitivity to allergens, and infants with eczema may also have allergies. In approximately 1 in 10 infants, eczema is made worse or triggered by a food allergy (commonly diary produce or eggs), which is why it most commonly appears around the time solids are introduced.
- Inflamed Ear Canal: Inflammation of the outer ear canal, the tube between the eardrum and the visible outer ear is also known as otis externa. It can be caused by infection with bacteria or fungi or can result from an allergy. It can also occur if eczema or another skin condition irritates the ear, prompting the child to scratch it, leading to infection. Take your child to the doctor who will prescribe some anti-inflammatory ear drops.
- Food Allergy: If you notice any of the following symptoms as you introduce solid foods to your baby, he or she may have a food allergy: skin rashes, nausea, diarrhoea, bloating, runny nose, watery eyes, itching, wheezing and difficulty breathing. Unlike a food intolerance, the symptoms of a food allergy occur quickly after eating the food, and, in severe cases, the allergy may cause a very serious and even life-threatening reaction known as anaphylactic shock. A food allergy occurs when the immune system mistakes a foodstuff for something harmful and attacks it. The reaction causes the body to release histamine and other chemicals that cause the aforementioned symptoms of an allergic reaction. Even a tiny amount of the food can prompt a reaction. Common allergy-inducing foods include dairy products, fish, nuts, eggs, tomatoes and citrus fruits.
 |
| Diagram showing the order in which teeth erupt. |
 |
| Baby eczema. |

7 Months:
- Meningitis: Meningitis is an infection of the lining of the brain. Infection with meningococcal bacteria is very serious as they can cause septicaemia (blood poisoning). If you are concerned that your child may have meningitis or septicaemia, seek urgent medical help.
- Bronchiolitis: In bronchiolitis, the small airways in the lungs (bronchioles) become infacted and swollen, which can cause difficulties breathing. It is usually a mild illness and most commonly affects babies. About 1 in 3 children have had bronchiolitis by the time they are one year old, with most being affected between 6 and 9 months (Kaye 2012).

9 Months:
- Blephartis: Blephartis is a very common condition. Babies who are affected are often bothered by persistently sore, gritty eyes and eyelids. The edges around the eyes become inflamed with crusts around the eyelashes. Conjunctivitis can be present concurrently.
- Flat Feet: If a child has flat feet it means that the soles of his feet rest on the ground, as if the normal arch of the foot does not exist. An affected child may feel some pain beneath the ankle and along the instep. Flat feet are normal in toddlers up to the age of 2 or 3 (Murkoff 2010).
- Rumination: Rumination disorder is an eating disorder in which a baby brings back up and re-chews partially digested food that has already been swallowed. In most cases, the re-chewed food is then swallowed again; but occasionally, the child will spit it out. To be considered a disorder, this behavior must occur in children who had previously been eating normally, and it must occur on a regular basis - usually daily - for at least one month (Dugdale 2012). The child may exhibit the behavior during feeding or right after eating. Symptoms include weight loss, bad breath and tooth decay, repeated stomach-aches and indigestion, and raw and chapped lips. In addition, infants with rumination may make unusual movements that are typical of the disorder. These include straining and arching the back, holding the head back, tightening the abdominal muscles, and making sucking movements with the mouth. These movements may be done as the infant is trying to bring back up the partially digested food.

10 Months:
- Impetigo: An extremely contagious bacterial skin infection, impetigo is common in young children, especially crawling babies. It generally appears around the nose, mouth, ears, and the diaper area. Visually impetigo looks like red, scabby patches of skin with honey-coloured crusts. The bacteria that cause impetigo enter through cuts, bites or scratches. Symptoms start 4-10 days after infection. See your doctor if you think your child has impetigo; an antibiotic cream will be prescribed.
- Ear Trauma: This is most commonly due to the use of cotton buds (Q-tips) which can cause inflammation and infection, but worse, can cause perforation of the eardrum, resulting in loss of hearing. Sometimes this damage cannot be repaired. Infection can also occur due to the insertion of a foreign body, as babies tend to experiment at this age. If you think your child has a foreign body in the ear, do not try to remove it. Consult your doctor.
- Nose Bleeds: As soon as babies discover how to pick their nose, the risks of nose bleeds increase. Nosebleeds are generally due to bleeding from blood vessels on the lower part of the septum (wall dividing the nostrils). These blood vessels are delicate and bleed easily. If your child’s nose is bleeding after an injury or if they are getting very regular nosebleeds (one per week or more), see your doctor.
- Halitosis: Halitosis (bad breath) can occur when the child has a foreign body stuck up their nose (yep, more fun with foreign bodies). If you suspect this may be the case with your child, see your doctor.
 |
| Impetigo. |

12 Months:
- Toddler’s Diarrhoea: Persistent diarrhoea that often contains recognizable pieces of food such as raisins, carrots, peas and beans, is most commonly due to toddler’s diarrhoea. The cause of toddler’s diarrhoea is not clear (Powell and Jenkins 2012). The child is generally well, has no fever, is eating and drinking, is active and growing as normal. Nonetheless, you may wish to see your doctor to rule out other causes of diarrhoea.
- Toddler Constipation: The average toddler makes a bowel movement once a day (Benaroch 2012). Usually, a child who has a bowel movement fewer than three times a week (or less often than normal), and whose stools are hard and difficult to pass is constipated. Don't be worried if your child has a bout of constipation -- it's perfectly normal once in awhile. But if your toddler's constipation lasts for two weeks or more it's called chronic constipation, and you should see your doctor.
- Gingivostomatitis: Gingivostomatitis is most common in toddlers and causes very painful ulcers to appear in the mouth. It results from a first infection by the herpes simplex virus, which also causes cold sores. Symptoms of gingivostomatitis include a fever, painful ulcers on the gums and swelling of the lymph nodes in the neck. If your child has these symptoms take her to see your doctor who may prescribe an antiviral drug.
- Febrile Convulsions: These are seizures that sometimes occur in children who have a high fever due to an infection. They most commonly affect toddlers during the first day of illness. The cause of febrile convulsions is not clear. Although they occur with a high fever, they may not be caused by the fever as keeping a child’s temperature down does not prevent them. They do run in families however, so if you or your partner had febrile convulsions as a child it is more likely that your child may have them (Sadleir 2007). In most cases, febrile convulsions last less than 15 minutes and do not reoccur during the child’s infection. If a seizure lasts longer than 15 minutes and it recurs several times during an infection it can indicate a more serious illness.
 |
| Gingivostomatitis. |
14 Months:
- Bow-Legged: It’s normal for toddlers to be bow-legged when they begin walking and running. This generally resolves by the age of 3 (Leah 2012). If the condition only affects one leg, see your doctor.
- Joint Infection: Infection of a joint is most common in toddlers up to the age of 2 years. The joint becomes inflamed and fluid collects within it. If treatment is delayed, the cartilage that covers bones inside the joint may be damaged, causing stiffness and deformity of the joint.
- Cuts and Grazes: Active, developing toddlers will fall and hurt themselves, and cuts and grazes are very common at this age. A cut is a split in the skin, while a graze, or abrasion, means layers of skin are scraped off (yep, you winced when you read that, didn't you?). Most minor cuts and grazes heal without scarring. You should seek medical advice if the wound will not stop bleeding, cannot be cleaned, or is very deep.
- Pigeon Toes: Inward rotation of the whole leg from the hip is the most common reason for a child to have pigeon toes, also known as in-toeing. Consult your doctor if you are worried. Pigeon toes usually improve without treatment by the age of 3 or 4 years (Collins 2009).
- Croup: A barking cough characterizes this viral infection of the voice box (larynx) and windpipe (trachea). It mainly affects toddlers (Kaye 2012). Children catch it by breathing in the droplets from affected people’s coughs and sneezes, or by touching an infected surface and then their mouths. In the UK, about six in every 100 children will get croup each year (BUPA 2012). It mainly affects children between the ages of a few months and six years old, but it is most common in toddlers. This is because at this age, children's windpipes and airways are smaller and so they are more likely to become narrower if they are infected. For this reason, the symptoms are usually more severe in younger children. If you suspect your child has croup, take her to your doctor for confirmation.

 |
| The sites of common respiratory illnesses in infancy. |
16 Months:
- Lick Eczema: A child with lock eczema has a rash around his or her mouth. The rash is caused by saliva irritating the lips and surrounding skin as a result of excessive lip-licking or thumb-sucking. Lick eczema clears up when the habit causes it disappears. Lip salve can help to protect your child’s lips from irritating saliva and also relieves the discomfort.
 |
| Lick Eczema. |
18 Months:
- Splinter: Toddlers who are continually exploring and touching everything frequently get splinters. These are often wood but can be glass, metal or plastic. You should attempt to remove splinters with tweezers to prevent an infection developing.
- Middle Ear Infection: Infection of the middle ear, which is located between the eardrum and inner ear, is a common cause of earache in small children. Also known as otitis media, the infection may be acute (short-lived) or longer lasting or recurrent (chronic). Young children are more likely than older children and adults to develop middle-ear infections because their Eustachian tubes are shorter and more horizontal, so it is easier for an infection to spread along them. Also, enlarged tonsils or adenoids, more common in young children, can block the Eustachian tubes. Children who were formula fed are more likely to develop a middle ear infection (Stuebe 2009).
- Glue Ear: In glue ear, also called otitis media with effusion, there is a build-up of a sticky fluid in the middle ear, hence the name glue ear. The exact cause of glue ear is not known but it may be due to a problem with the Eustachian tubes that prevents them from draining fluid away from the middle ear. Medical treatment is not normally required as the condition normally clears up within 3 months, however visit your doctor if you become concerned about your child’s hearing (NHS 2013).
- Limping: A limp is usually caused by a minor injury that will get better on its own. It could, however, be caused by an underlying disorder (e.g. irritable hip, bone or joint infection, muscle strain, juvenile chronic arthritis) that requires prompt treatment to prevent permanent disability. Never ignore a limp in a child. See your doctor.
- Threadworms: Infection of the intestines with threadworms is common in young children. These tiny worms (a few millimetres long) lay eggs around the anus (as many as 10,000), which causes intense itching. Threadworms are caused by swallowing eggs laid by female worms. This can happen if a child touches the hands of an infected person whose hands are contaminated with eggs, and then transfers the eggs to their mouth. Children who suck objects are mostly affected (Collins 2009). If you suspect your child has threadworms, see your doctor.
- Rickets: This condition causes the bones to become soft and malformed, which can lead to bone deformities. The most common cause of rickets is a lack of vitamin D and calcium. Symptoms include bone pain, delayed growth, skeletal problems, or still being unable to walk at 18 months (Hudson 2002). If your child has any of these symptoms, see your doctor.

 |
| Illustration of thread worms around the anus. |
2 Years:
- Measles: This viral infection can be extremely serious, even fatal. The first signs of measles are a fever, cough and cold symptoms, followed by a rash of red spots. The spots of the measles rash often join together, creating red patches. The rash spreads over the face and body (see photo). Measles is one of the leading causes of death among young children (WHO 2013). If you think your child has measles, notify your doctor immediately.
- Urinary Tract Infections: Infections of the urinary tract are caused by bacteria. They rear their ugly head more often around the time of toilet training. They are more common in girls because the urethra, the tube that carries urine out of the body, is shorter than in boys, so bacteria don’t have so far to travel to reach the bladder. In girls, urinary tract infections can be caused by wiping their anus from back to front after a bowel movement. If your child has symptoms of a urinary tract infection, they should be seen by your doctor.
- Infective Conjunctivitis: This is inflammation of the conjunctiva, the transparent membrane that covers the white part of the eye and the inner eyelids. In toddlers, infective conjunctivitis is most often caused by a virus. It is caught by being in close contact with an infected person and is very contagious. Most cases of infective conjunctivitis are mild and do not require medical treatment as they get better within a few days. Studies have shown that dispensing breast milk into the child’s affected eye can speed up the recovery process (Verd 2007; Baynham 2013).
- Pnemonia: Pneumonia is a type of chest infection in which the air sacs in the lungs (alveoli) become infected and fill with fluid, resulting in a cough and difficulty breathing. Prompt treatment is important. People of any age can develop pneumonia, although toddlers are at higher risk. Pnemonia is also common in parents who spoke. Children who were formula fed are more likely to develop pneumonia (Stuebe 2009).
- Vaginal Problems: Inflammation of the external genitals (vulva) and the vagina is a common problem in girls who are learning to use the toilet. It is also known as vulvovaginitis. Young children frequently don’t wipe themselves properly (Cave and Fertleman 2009). Wiping from back to front after using the toilet can cause soreness, itching and vaginal discharge. If these symptoms persist or are severe, take your child to your doctor who may prescribe antibiotic cream.
- Mumps: Mumps is a viral infection that causes swelling of salivary glands in the cheeks. It is caught by breathing in the virus in droplets from infected people’s coughs and sneezes. Symptoms appear 2-3 weeks after being infected. If you think your child has mumps you should notify your doctor.
- Orchitis: This inflammation of the testis most often occurs as a complication of mumps. Orchitis is also commonly caused by a bacterial infection. It is not serious, and usually disappears within a week. Symptoms include pain in the testis and sometimes a fever. If your son has not had mumps within the past few weeks, seek urgent medical help to rule out a more serious condition called testicular torsion (Bullock et al 2007).
- Hand, Foot and Mouth Disease: This common mild viral infection, which lasts about a week, causes small ulcers to appear inside the mouth. It is contracted by breathing in droplets containing the virus. Symptoms appear 3-6 days after infection and usually clear up in 7-10 days. If the spots become infected through scratching see your doctor who may prescribe antibiotics.
- Obstructive Sleep Apnoea: Apnoea is a pause in breathing. In obstructive sleep apnoea (OSA), pauses occur during sleep as a result of blockage in the upper airways. The pause causes the child to wake slightly so that breathing starts again, but sleep has been disturbed. In children, obstructive sleep apnoea can be caused by large tonsils or adenoids blocking the passage of air to the lungs. A child who is overweight is at increased risk (Arens and Muzumdar 2010). Sleep apnoea affects about 1 in 50 children, most commonly those aged between 2 and 7.
- Ringworm: Ringworm doesn’t refer to a worm but is a fungal infection that can affect the skin of the body and or the scalp. It’s called ringworm because it produces a ring-shaped rash on the skin. It is very common. 10-20% of people will have some form of ringworm at some point of their lives (NHS 2013), however you children are particularly susceptible to it. Ringworm spreads easily between people by direct contact. They can also be spread from animals and from indirect contact, from fungal spores found on towels and sheets. Your pharmacist can treat ringworm with antifungal creams.
- Epiglottitis: This is a serious condition that can cause difficulties in breathing due to swelling of the epiglottis, the structure that covers the trachea (windpipe) during swallowing to prevent food from entering the lungs. Epiglottitis is caused by an infection, most commonly the Hib virus and can sometimes be a complication of croup. It can affected people of any age but is more common in non-vaccinated children between the ages of 2 and 7 (Jackson 2012). Epiglottitis is a medical emergency so call an ambulance.
- Dairy Intolerance: When a child has a dairy intolerance, they lack a specific enzyme needed to break down dairy foods. Babies normally have high levels of the enzyme lactase, which breaks down lactose. But sometimes after age two the levels of this enzyme fall too much, causing symptoms of intolerance when dairy is consumed (Saville and Sullivan 2003). Symptoms include nausea, abdominal pain, bloating and diarrhoea.
- Constipation: Around this age, constipation is common. The average 2-year-old is far more interested in playing with toys than in going to the bathroom. Some children are embarrassed or afraid to use the toilet, especially when it's a public restroom. Toddlers who rebel against the toilet training process sometimes express their power struggle in a refusal to go. Constipation often only lasts a few days. If it lasts longer than a week, see your doctor.
- Trichotillomania: Trichotillomania is hair loss caused by the child pulling, plucking, twisting, or rubbing his or her hair. The hair loss is patchy and characterized by broken hairs of varying length. Patches are typically seen on the side of the child's dominant hand. Trichotillomania may be triggered by a stressor or anxiety (Walther et al 2013).
- Meckel's Diverticulum: This fascinating condition is characterised by a slight bulge in the small intestine which is present at birth. This bulge has its own blood supply and is actually a remnant of the yolk sac that was present during embryonic development. It is the most common malformation of the gastrointestinal tract and is present in approximately 2% of the population (Stallion and Shuck 2001). Most people are unaware that they have the condition, however for some children, at around 2 years old symptoms begin. The most common are: rectal bleeding, smelly black stools, and stomach pain. In most cases bleeding occurs without warning and stops spontaneously. Consult your doctor immediately if your child shows any of these symptoms. If they are found to have Meckel's Diverticulum, surgery may be advised.
- Irritable Hip: This condition occurs when the lining of the hip joint becomes inflamed and fluid accumulates inside the joint. The cause is unknown, but irritable hip often develops within about 2 weeks of a mild upper respiratory tract infection, such as a cold. Children aged 2 to 12 years are most susceptible to irritable hip (NHS 2013). Symptoms include pain in the hip, groin, or knee, and sometimes a mild fever. Bed rest and painkillers such as paracetamol, will be advised by your doctor.
- Henoch-Schonlein Purpura: In Henoch-Schonlein Purpura, small blood vessels become fragile and allow blood to leak from them. Bleeding into the skin results in an easily identifiable rash, while leakage of blood into joints, the kidneys, or the digestive tract causes various other symptoms. The disease is fairly common in children between the ages of 2 and 10 years, and is not usually serious. The cause is unknown, but may involve an allergic reaction or bacterial infection (Qandeel and Fenton 2013). Consult your doctor who will direct blood tests.
 |
| Measles rash. |
 |
| Mumps swelling. |

 |
| Ringworm. |

3 Years:
- Knock-Kneed: Around this age children commonly become knock-kneed. This generally resolves itself, though it can take a little while. If the condition only affects one leg, see your doctor (Kaneshiro 2012).
- Giardiasis: A digestive tract infection that causes diarrhoea, fever, nausea, abdominal pain and burping, giardiasis is caused by a tiny parasite which can live for long periods outside the body. The parasites can be spread by poor hand-washing after using the toilet and then touching other people. If you think your child may have giardiasis you should see your doctor who will request a stool sample (the things we parent's gotta do).
- Bone Infection: Children aged 3 to 14 years, especially boys, are susceptible to bone infection (POSNA 2011). The long bones of the arms and legs are most often affected. Without prompt treatment, bone infection may become chronic and difficult to eradicate. Symptoms include severe pain in the affected arm or leg, which the child is reluctant to move or allow to be touched, accompanied by a fever.
- Molluscum Contagiosum: This viral infection causes shiny, raised spots to appear on the skin. It commonly affects young children and spreads easily at preschool and school. Molluscum contagiosum is caused by a pox virus and spread by direct contact with the skin of an infected person or by sharing towels or even toys. The lesions generally clear up on their own.
- Influenza (Flu): Influenza is a viral infection which affects the lower respiratory tract. There are three main types, A, B and C. Influenza A and B cause the most infections. Flu is transmitted through droplet infection, when those with the infection cough or sneeze. They may also pass germs by touching shared things such as toys or door handles. The common symptoms of flu are: appetite loss, lethargy, headache, painful muscles and joints, fever, dry cough. In many countries a seasonal flu vaccine is offered to all preschoolers. Contrary to popular belief, a child does not have to suffer from a chronic medical condition, in order to face increased risk of death. Between 2004 and 2010, among the kids killed by the flu, 35 percent had no chronic medical condition (Pediatrics 2013).
- Scabies: Scabies is a skin infestation by tiny mites called Satcopte scabei that can’t be seen by the naked eye. The mites burrow under the skin to lay their eggs, causing intense itching. Scabies are spread by close physical contact and can also be passed on by sharing towels and bedding as they can live for short periods without a host. If you think your child has scabies, visit your doctor who will prescribe a cream or lotion.
- Gastroenteritis: Bouts of gastroenteritis – an infection of the stomach and intestines – are extremely common in children. Viruses can be picked up by touching an infected person who hasn’t washed their hands properly after using the toilet, or by touching an object an infected person has touched, then transferring the virus or bacteria to the mouth. Children who were formula fed are more likely to develop gastroenteritis (Stuebe 2009).
- Sinusitis: This condition is an inflammation of the lining of the sinuses (air-filled cavities in the bones that surround the nose). Sinusitis is more often caused by bacterial infection following a cold when mucus produced in the sinuses traps bacteria. Symptoms include: runny nose, feeling of fullness in the cheeks, cough, headache, pain in back teeth, loss of sense of smell, and sometimes a fever.
- Chickenpox: Children of this age are especially likely to catch chickenpox, although the disease can occur at any age. Usually a mild and short-lived illness in children, it causes a distinctive rash of extremely itchy spots that turn into blisters, then crust over. Chickenpox is more common in the spring. It takes 10-21 days for symptoms to develop after being injected. Your child is infectious for 2 to 3 days before until 5 days after the rash appears. Unless your child is particularly unwell, chickenpox does not usually require medical care (Kaye 2012).
- Whooping Cough: Also known as pertussis, whooping cough is a bacterial lung infection that causes intense bouts of coughing that may end in a whooping sound. It is extremely infectious and is spread by breathing in droplets from an infected person’s coughs and sneezes. Symptoms appear 7-10 days later. Immunity to whooping cough does not last forever - even if a person is vaccinated for protection or has had the disease before (Brown 2013). If you think your child has whooping cough, you should consult your doctor who will prescribe antibiotics.
- Headlice: Another common preschool infestation, headlice are wingless insects that live on the scalp and bite the skin to feed on blood. They are tiny – about 2-4mm long – and so can be difficult to detect. They can make the scalp extremely itchy. Although anyone can catch headlice, they are more common in children who spend a lot of time together playing in close proximity. If your child has headlice your pharmacist will be able to recommend a treatment.
- Enlarged Adenoids: The adenoids, which are at the back of the nose, are part of the body’s infection-fighting system. They can become enlarged in young children causing noisy breathing, snoring, bad breath and ear infections. Often no treatment is needed as the symptoms are mild. As your child grows and develops, the adenoids generally shrink so symptoms improve. If your child’s symptoms are severe, for example, if they are affecting sleep or she gets glue ear regularly, surgery to remove the adenoids may be recommended.
- Common Cold: The common cold is a viral infection of the nose, throat, and sinuses (the upper respiratory tract). It is extremely common, especially in children, with the average child having at least six colds a year, more when they start preschool (Kaye 2012; Collins 2009). Children most commonly catch colds from other children, which means that the preschool years herald the beginning of a long journey of cold-catching. Here, children are exposed to a wide variety of viruses to which they have not yet built up immunity.
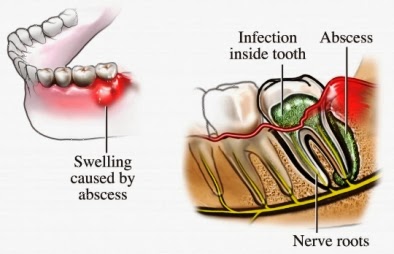
- Dental Abscess: At this age children develop a hankering for candy and are also entering environments (preschool and other childcare) where parents are unable to regulate their diet. If a child develops tooth decay, the enamel of the tooth is broken down and bacteria in the mouth can infect the soft tissues at the centre of the tooth (the pulp) and spread down to the bone surrounding the root. If you think your child may have a dental abscess, seek dental help urgently. Your dentist will probably release the pus in the abscess by drilling into the tooth to remove the infected pulp. If a milk tooth is affected, it may be removed.


 |
| Satcopte scabei laying eggs under the skin. |


4 Years:
- Warts and Verrucas: When children begin formal schooling they often get warts, which are harmless growths on the skin. There are two main types: common warts, which occur anywhere on the body, but more often on the hands, and veruccas which occur on the soles of the feet. The virus is found within the skin cells of the wart and is passed on by direct contact, or indirectly, for example by sharing shoes, towels, or washcloths, or by walking over floors someone infected by the virus has walked over, as at swimming pools. About 50 percent of warts go away untreated, but others need a doctor's attention (Fraiser et al 2007).
- Epiglottitis: This is an inflammation of the epiglottis, the flap of cartilage at the entrance of the trachea that closes when a child swallows. It mainly affects young children of school-starting age (Collins 2009). If your child has difficulty swallowing and breathing, call an ambulance immediately.
- Eyesight Problems: Studies suggest that one six-year-old in 20 has an uncorrected eyesight problem (Byron 2006). Before your child starts school is an excellent time for an eye test as this can pre-empt problems in class. Don’t wait for symptoms such as straining to see the TV or squinting at books before taking your child to see the optician.
- Scarlet Fever: Scarlet fever is a bacterial illness that causes a distinctive widespread pink-red rash that feels like sandpaper to touch. It may start in one area, but soon spreads to many parts of the body, such as the ears, neck and chest. The rash may be itchy. Other symptoms include a high temperature, a flushed face and a red, swollen tongue. Scarlet fever is extremely contagious and can be caught by breathing in bacteria in airborne droplets from an infected person's coughs and sneezes; skin to skin contact; and sharing contaminated towels, baths, clothes or bed linen. Ninety percent of cases occur in children 3 to 8 years old (Cox and Sallis 2009). See your doctor if you suspect your child may have scarlet fever. It can be easily be treated with antibiotics.
- Travel Sickness: Feeling sick when travelling by car, sea, or air is common in children of this age. Although nearly 80 percent of the general population experiences motion sickness at one time in their lives, children between the ages of four and ten are most vulnerable (Davidson et al 2013). Travel sickness is thought to be due to a mismatch between information supplied to the brain from the eyes and the balance system in the inner ear.

 |
| Rough, swollen tongue, typical of Scarlet Fever. |
5 Years:
- Tonsillitis: Tonsillitis is inflammation of the tonsils, usually due to a viral infection or, less commonly, a bacterial infection. Symptoms of tonsillitis include: sore throat that can feel worse when swallowing, fever, coughing, and headache. Tonsillitis is very common in children aged 5-15 years old. Almost all children will have at least one episode of tonsillitis as they grow up (NHS 2012). Symptoms will usually pass within 3-4 days.
- Abdominal Migraine: Children, often between the ages of 5 and 9, sometimes get a form of migraine that causes abdominal pain rather than a headache. Certain triggers may bring on abdominal migrane, such as foods, additives, exercise, or stress. If your child is showing these symptoms, it is important to see your doctor so that other causes can be ruled out.
- Losing Teeth: Usually milk teeth only start to fall out when secondary teeth are coming through. A wiggly tooth will be exciting for your child because it is a sign of growing and she will know that the tooth fairy might visit. It may, however, also make her anxious because a loose tooth can be painful and cause the gum to bleed. The process can linger too, with the tooth hanging on by a strand for days.
- Iron Deficiency: Iron deficiency anaemia is common at this age and has been shown to cause problems such as poor behaviour, slow growth, tiredness, and recurrent infections (Byron 2006). If your child looks pals and seems excessively tired, she may be anaemic and you should see your doctor.
- Growing Pains: Beginning now, so-called ‘growing pains’ are common. Your child might complain of intermittent leg or arm pains, often during the night. Not all pains are growing pains: being stressed, minor injuries, infections, and even juvenile arthritis can also cause limb pain. If your child’s symptoms are persistent, see your doctor.
- Hearing Loss: Some five-year-olds have undiagnosed hearing problems, as the result of repeated ear infections, or for no obvious reason. Hearing loss can be hard to detect, because hearing can fluctuate from day to day. But it is vital to spot it, as this is a crucial time for your child’s learning. If you suspect there may be a problem, see your doctor for a hearing test.
- Nephritis: Nephritis is a disease that affects the kidneys, and it develops after a streptococcal infection such as tonsillitis. To combat this infection the body produces antibodies but, due to a defect in the body’s immune system, these antibodies may go on working after the infection has passed and begin to harm the kidneys, which become inflamed. The condition comes on suddenly in children and produces symptoms of reddish-brown urine and mild swelling of the face, ankles and abdomen. Nephritis accounts for 10 to 15 percent of all hospitalizations due to kidney failure in the United States (Jovinelly 2012). Consult your doctor immediately if your child is exhibiting any of these symptoms.
- Appendicitis: Appendicitis is a painful swelling of the appendix, a finger-like pouch connected to the large intestine. It's located in the lower right-hand side of the abdomen. The condition normally affects children over the age of five. It starts as a pain in the centre of the abdomen. It then travels to the lower right-hand side and gradually gets worse. Appendicitis is a medical emergency that usually requires urgent surgery to remove the appendix. In 20 to 30 percent of children, the appendix ruptures and releases the infection into the abdominal cavity (Cleveland Clinic Foundation 2013).


6 Years:
- Pityrasis Alba: In pityriasis alba, patches of lighter coloured skin develop, often on the face. 63% of cases occur on the forehead (Guareschi and Lernia 2009). It generally affects children aged 6-12 and disappears on its own. No treatment is necessary.
- Encopresis: If a child frequently passes solid stools in his pants or in inappropriate places after he has bowel control, he has encopresis. The condition affecting boys three to six times more often than girls (American Psychological Association 2013). The most common cause of encopresis is chronic constipation. If you can find no reason for the involuntary soiling, consult your doctor who can carry out tests.
- Perthes’ Disease: This condition affects some children, particularly boys, around this age. Poor blood supply causes progressive softening, followed by reforming and hardening, of the head of the thigh bone, or femur. Symptoms include pain in the hip or knee and restricted movement. Perthes’ disease will get better spontaneously within 2-4 years. About 60 percent of children recover without any treatment but monitoring is essential in order to prevent the hip joint from becoming deformed (Oxford University Hospital 2013).
- Phimosis: Phimosis is the name given to an abnormal tightness of the foreskin which prevents it from being drawn back over the tip of the penis. Phimosis can cause problems with urination, however in most cases the problem fixes itself as most foreskins will naturally become retractile by adulthood (McGregor et al 2007).
 |
| Pityriasis Alba. |
7 Years:
- Bladder Control Problems: As they get older, children gain bladder control and generally are dry in the day first, then at night. If a child is not dry in the day and night by age 7, seek medical advice. Bed-wedding can occur because a child sleeps very deeply and the part of the nervous system that tells him to wake up and go to the toilet is immature. It can also occur because the body does not yet produce enough antidiuretic hormone, which reduces hormone production at night. If you wet the bed yourself after the age of 7, your child is also more likely to do so (Von Gontard 2001; Arnell 1997). A child who is wetting again after having been dry in the day or night could have an underlying medical condition or be suffering from stress or anxiety.

8 Years:
- Precious Puberty: The average age for a girl to start puberty is around age 10 to 11 years, and the first signs are generally breast changes. The average age for a boy to start puberty is around 12 to 13 years, with the testes enlarging in size. In precocious puberty, these changes take place abnormally early. While in general precocious puberty is much more common in females than males, hereditary forms are more common in males (Kaplowitz et al 2013). If you suspect your child is starting puberty around now, take them to your doctor for an assessment.

9 Years:
- Osgood-Schlatter Disease: In this disorder, there is inflammation of the tibia (shinbone) just below the knee at the point where a large tendon is attached. Osgood-Schlatter mainly effects boys aged between 9 and 14 years. The main symptoms are tenderness, pain, and swelling just below the knee, which usually worsens with exercise. Your child should be seen by a doctor, who will probably refer him or her to an orthopaedic surgeon.
 |
| Osgood-Schlatter Disease. |
10 Years:
- Pityriasis Rosea: This skin rash, consisting of pink oval patches, is most common in children aged 10 or older, but can occur in younger children. Its cause is not known, however up to 69 percent of patients have illness symptoms before the patches appear (Stulberg and Wolfrey 2004). Pityriasis Rosea does not appear to be infectious and generally disappears on its own within about 8 weeks. Most commonly affected areas include the trunk, arms and legs.
- Over-Exercising: Some children of this age will be sports enthusiasts and exercising should be applauded – it helps to strengthen muscles and bones and benefits the cardiovascular system. However, it is possible for children to over-exercise and sports such as gymnastics can put too much stress on joints and muscles. Sometimes children become exercise fanatics to keep themselves thin as part of an eating disorder and as a result pubertal development may be delayed.
- Psoriasis: This chronic skin condition rarely affects children under 10 years old. The rash does not usually itch, but can be uncomfortable and the look of it may upset your child. It tends to vary in severity and often gets worse during illness or emotional stress. Psoriasis cannot be cured and is likely to recur, but individual attacks can be controlled with proper treatment.
 |
| Pityriasis Rosea. |
11 Years:
- Sever's Disease: This is a painful bone disorder that results from inflammation (swelling) of the growth plate in the heel. During the growth spurt of early puberty, the heel bone sometimes grows faster than the leg muscles and tendons. This can cause the muscles and tendons to become very tight and overstretched, making the heel less flexible and putting pressure on the growth plate. Over time, repeated stress on the already tight Achilles tendon damages the growth plate, causing the swelling, tenderness, and pain of Sever's disease. Such stress commonly results from physical activities and sports that involve running and jumping, especially those that take place on hard surfaces, such as track, basketball, soccer, and gymnastics. In 60 percent of the cases, it affects both heels (NHS 2011).
- Stress: The emotional impact of puberty, combined with school examinations, can cause many pre-teens to suffer from stress. One in three 11 year-olds report feeling 'upset, depressed, angry or stressed' (The Telegraph 2009). Common symptoms of are headaches, stomach aches, and sleep disturbances, mostly due to anxiety rather than an underlying condition. They are all very real symptoms and are due to the over-production of the hormones that are produced by stress interacting with the body.
- Period Pains: Most girls start their periods between the ages of 10 and 16, so by age 11 your daughter should be well prepared for what to expect. Unless she is extremely fortunate, your daughter is bound to have period pains. These are a normal part of menstruation, occurring when the walls of the uterus contract. Painkillers and a warm bath can help.
- Heavy Periods: Most girls will get heavy periods (menorrhagia) at some point (Byron 2006). This is bleeding that soaks through a sanitary pad each hour for a day or two, or which lasts longer than seven days. There are often large clots. If this happens regularly, it may be due to a hormone imbalance and treatment is available.
 |
| The site of pain in Sever's Disease. |
12 Years:
- Malocclusion: Malocclusion is a poor fit between the upper and lower teeth when they bite together. Treatment is needed only if the teeth are so crooked or out of position that they look unsightly or are difficult to clean, so increasing the risk of tooth decay or gum problems. The most common cause is the overcrowding of the teeth, a problem suffered by two out of three 12 year old children (Collins 2009). A brace may be required. Up to 70 per cent of all children need some sort of orthodontic treatment at some point (Byron 2006). Such treatment works best and is least painful at this age.
- Headaches and Migraines: Your child may get headaches and the most common causes are stress and mild dehydration, although they may also be due to migraine, sinusitis and eye problems. Only one child in 40,000 is found to have a brain tumor causing the headache (Children's Hospital of Wisconsin 2013). Migraine often runs in families and is due to a temporary alteration in blood flow to the brain, which causes a severe headache, and is usually one-sided. It may also temporarily affect vision and cause nausea and vomiting. If your child shows no improvement after taking painkillers, see your doctor.
 |
| Severe Malocclusion. |
Contact Dermatitis: Dermatitis (inflammation of the skin) resulting from contact with irritating substances does not often occur in children until around 12 years. Common irritants include nickel (found in jewellery), rubber, fabric dyes, plasters, plants, bubble baths, detergents, medicinal creams, and cosmetics. Symptoms of dermatitis include an inflamed, scaly rash, intense itchiness, and sometimes blistering and weeping.
13 Years:
- Scoliosis: This condition, which can be genetic, causes an abnormal sideways curvature of the spine. Scoliosis can be due to a structural abnormality of one or more vertebrae or to a local muscle weakness. It is most common in girls. Starting around 13 years, when they experience the adolescent growth spurt (Wild et al 2013). Consult your doctor if you see a curvature in your child’s back when he or she stands up and bends forward.
- Lethargism: Adolescence in our culture is a recipe for sleep deprivation. Even without taking cultural factors into account, adolescents’ night-time sleep is shallower and less restorative than the sleep of younger children (see Timeline of Baby and Toddler Sleep), and the ability to nap during the day returns. Thus, even under the best conditions, a teenager is sleepier in the daytime than she was as a child. At the same time, she is better able to fight off sleep and stay up late. She also develops the ability to ‘oversleep’ – to sleep longer than she actually needs. Finally, some evidence suggests that adolescents have an inherent sleep-phase delay: they naturally fall asleep and wake later in the day, relative to light exposure, than younger children do (Ferber 2013).
- Acne: It is normal for teenagers to get acne. These unsightly and often painful spots can occur on the face and on the body. Acne is caused by an abnormal response in the skin to the hormone testosterone. The pores in the skin become blocked by oil and this causes spots. Severe acne can be genetic.
 |
| Scoliosis of the spine. |
14 Years:
- Eczema: Eczema is a common skin problem in children, flaring up at various points throughout childhood (see: age 6 months). Flaring tends to occur at times of stress and, especially in teenagers, may also be triggered by cosmetics, perfume and hair dye (NHS 2012).
- Delayed Puberty: Puberty is considered delayed if your daughter has no breast buds or pubic hair developing by the age of 14, or if your son has not had any of the signs of pubertal development by the age of 14 (Collins 2009). In both instances, see your doctor.
- Pityriasis Versicolor: An overgrowth of yeast normally present on the skin, possibly triggered by exposure to sunlight or a hot, humid environment, causes the discoloured patches of this skin condition. It is rare in children before the start of puberty. Although it is not harmful or contagious, the condition may persist indefinitely if not treated. See your doctor if you think your child has this condition and an antifungal cream will be prescribed. 97% of patients seem improvement with treatment (Vicik et al 1984).
- Athlete’s Foot: This easily treated fungal infection affects the soft area between and underneath the toes. At an advanced stage, it also affects the nails. It is contagious and is usually picked up by walking barefoot in communal areas such as shower rooms, gymnasia and swimming pools, where infected feet have been. The infection is aggravated by sweaty feet because the fungus (tinea) thrives in warm, moist conditions. Yet another reason to make your teenage son wash his socks.
- Halitosis: Halitosis (bad breath) is a very common problem with teenagers. It can be caused by eating strong foods or by secret smoking. A teen who is crash-dieting can suffer too.
 |
| Eczema of the hand. |
15 Years:
- Chondromalacia Patellae: In this condition, the cartilage at the back of the patella (kneecap) becomes soft, swollen, and roughened. Girls aged 15 to 18 years are the group most susceptible to chondromalacia patellae. The main symptom is aching pain behind the kneecap. The pain is made worse by exercise (especially climbing stairs) and gets better with rest.
- Depression: In children, depression most often affects teenagers and can is an important cause of suicide. In fact, suicide, is the third leading cause of death in 15-24 year olds (ADAP 2013). The causes of depression are varied. Bereavement or exam stress are common culprits. Some types of depression run in families, and there may also be a biochemical factor. If your child’s depression deepens or persists for more than a few weeks, a doctor should see your child.
- Poisoning: The number of teens who abuse inhalants has doubled in the last decade (Settle and Price 1999). The risk is enormous because the effects of inhaling toxic chemicals are so unpredictable. Inhalants are commonly found in homes – glue, nail polish remover, tip-ex, felt-tip markers, lighter fluid, oven cleaners, hair spray, and furniture polish are just a few. As with other kinds of drug use, kids use inhalants for the stimulation or ‘high’. The American Academy of Paediatricians has listed several warning signs to look out for: A chemical smell, paint, or staining on clothing or the child’s body; Spots or sores around the mouth; A drunk glassy-eyed look; Nausea, loss of appetite; Anxiety, excitability, irritability.




Comments
Post a Comment